I see lots of clients whom are experiencing shoulder pain. The cause of the pain is commonly one of the below problems. Where possible I always try and treat the problem without surgery.
 Dislocation of the ball and socket joint can occur at any age but is usually the result of injury often sports related. In the younger age group this may result in recurrent dislocations and in the more mature individual tears in the muscles around the joint.
Dislocation of the ball and socket joint can occur at any age but is usually the result of injury often sports related. In the younger age group this may result in recurrent dislocations and in the more mature individual tears in the muscles around the joint.
Treatment for minor levels of instability is often helped by well directed physiotherapy. For more frequent dislocators an MRI scan will usually help direct me by showing the degree of damage. If possible I will repair the damage using keyhole techniques.
For individuals repair may need to be done using the addition of a bone block fixed to the front of the socket.
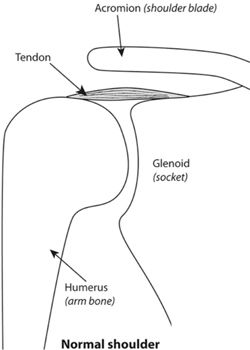
Rotator cuff tendinitis (bursitis/impingement)
The muscles of the rotator cuff surround the head of the humerus (ball) and held keep it snug on the socket. With increasing age or injury the space for the tendons to glide beneath the acromion can become narrowed resulting in them rubbing, becoming inflamed and painful.
Pain on taking the arm away from the body, reaching behind the back (arm in jacket, pulling up trousers, tucking shirt in) is common and is often worse at night. The pain travels down the arm to the elbow and at times may make overhead movement extremely painful.
Initial treatment will usually involve a cortisone injection to try and calm the inflammation and to allow physio rehabilitation. If this does not help it is possible to remove some of the bone off the undersurface of the acromion (sub acromial decompression) using keyhole surgery.
These may result from an acute injury or as a result of wear and tear over time. Pain on taking the arm away from the body is often associated in reduced power of this movement as well as a grating sensation when performing this action.
Not all need to be repaired but, for those who need surgery, reconstruction of the tendon and re-attachment to bone is achieved using small anchors inserted into bone with sutures over the top.
Frozen Shoulder (adhesive capsulitis)
This a condition which causes limited movement of the shoulder due to the lining of the joint becoming thickened binding the ball and socket preventing movement.
Some cases resolve spontaneously but others need releasing either by manipulation of the joint under anaesthetic or by using the keyhole technique to release the restriction.
Wear of the cartilage lining of the ball and socket joint of the shoulder is less common than the hip. Shoulder replacements have become much more reliable in the last ten years. I now perform at least 60 shoulder joint replacements each year. These operations provide reliable relief of pain and improvements in movement. I perform standard anatomic shoulder replacement as well as reverse geometry shoulder replacement.
Acromio-clavicular joint (ACJ)
Pain in this joint is usually felt on the top surface of the shoulder and may result from arthritis or injury. Treatment of pain is often successful with a cortisone injection. If this does not help then shaving out the joint using the telescope can be performed and is often combined with a subacromial decompression.
 A fall from height onto the shoulder may result in the joint between acromion and clavicle (shoulder blade and collar bone) being separated resulting in a visible bony lump above the shoulder. Not all these need surgery as many return to full funtion though the lump will remain.
A fall from height onto the shoulder may result in the joint between acromion and clavicle (shoulder blade and collar bone) being separated resulting in a visible bony lump above the shoulder. Not all these need surgery as many return to full funtion though the lump will remain.
Reconstruction of the joint using an artificial ligament results in leveling of the shoulders.